Effect of Staff Wellness Programs on Nurses’ Perceptions of Supporting Healthy Behaviors in R2 Healthcare Settings, Riyadh, Kingdom of Saudi Arabia
Premalatha Jayachandra*, Ahmed Al Rasheedi
National Neuroscience Institute Nursing Administration, King Fahad Medical City, Riyadh, Kingdom of Saudi Arabia.
*Corresponding Author’s Email: premjaya76@gmail.com
ABSTRACT
Background: Nurses commonly experience high levels of occupational stress that can negatively influence their emotional health, job performance, and the quality of patient care. Workplace wellness programs that include interventions such as counseling support, recreational activities, creative therapies, and lifestyle coaching have been introduced to improve well-being; however, evidence on their effectiveness in hospital nursing populations remains limited. Objectives: This study aimed to assess the impact of a Staff Wellness Program on reducing psychological distress and enhancing nurses’ perceptions of organizational support for healthy behaviors. Methods: A quantitative pretest–posttest design was carried out among registered nurses working across 12 hospitals in the Riyadh Second Healthcare Cluster (R2), Kingdom of Saudi Arabia, administered by King Fahad Medical City (KFMC). Participation was voluntary following institutional invitations. Due to logistical arrangements, baseline assessment and program implementation were conducted at PIMA Hospital during a Staff Wellness Day. Data were collected at baseline and three months post-intervention using a structured electronic questionnaire accessed via QR code with online informed consent. Psychological distress was measured using the General Health Questionnaire-12 (GHQ-12), while perceptions of healthy behavior support were assessed using a validated scale. Data analysis included paired t-tests, McNemar test, and Pearson correlation, with reliability confirmed using Cronbach’s alpha and intraclass correlation coefficients. Results: There was a statistically significant reduction in GHQ-12 scores after the intervention (mean difference = -3.88, p < 0.001), indicating improved psychological well-being. Healthy behavior perception scores showed a significant increase (mean difference = 9.14, p < 0.001), corresponding to a 16.22% improvement. Post-intervention findings demonstrated a transition from moderate to higher levels of positive perception, with an increase in the “very high” category (32.8%) and a reduction in the “low” category (6.8%). A significant inverse correlation was found between psychological distress and healthy behavior perception (r = −0.37, p = 0.01). Age emerged as the only demographic factor significantly associated with post-test distress levels. Conclusion: The Staff Wellness Program demonstrated effectiveness in reducing psychological distress and improving nurses’ perceptions of workplace wellness support. These results highlight the value of structured wellness initiatives in enhancing nurses’ psychological well-being and promoting positive workplace behaviors. Continued implementation of such programs is recommended to strengthen resilience, support well-being, and improve the quality of patient care.Keywords: Healthy Behaviors; Nurses; Psychological Distress; Staff Wellness Program
INTRODUCTION
Healthcare systems worldwide increasingly recognize the importance of staff wellness programs in promoting employee well-being, enhancing job satisfaction, and improving overall organizational performance. Nurses, who constitute the largest proportion of the healthcare workforce, are frequently exposed to high levels of occupational stress, long working hours, and emotionally demanding environments, placing them at increased risk of psychological distress, burnout, and unhealthy lifestyle behaviors.
Psychological well-being is a critical determinant of nurses’ ability to deliver safe, effective, and patient-centered care. Poor mental health has been associated with reduced work performance, increased absenteeism, higher turnover, and compromised patient safety and outcomes (Hussein et al., 2024) The General Health Questionnaire-12 (GHQ-12) is a widely validated tool used to assess psychological distress in healthcare settings. In addition to mental health, healthy behaviors including balanced nutrition, physical activity, adequate hydration, and stress management are essential for maintaining nurses’ overall well-being. However, demanding schedules and workplace constraints often hinder the adoption and sustainability of these behaviors.
An equally important factor is nurses’ perception of organizational support for healthy behaviors. This includes access to wellness resources, leadership support, and a conducive work environment. Positive perception is associated with increased engagement in wellness activities, improved job satisfaction, and better health outcomes, ultimately contributing to improved patient care quality (Alharbi et al., 2025). In Saudi Arabia, healthcare transformation initiatives have emphasized workforce well-being as a key component of quality improvement. The Riyadh Second Healthcare Cluster (R2) represents a major healthcare network where nurses face increasing workload demands, contributing to stress and burnout.
Despite the global expansion of staff wellness programs, limited evidence exists within the Saudi context, particularly regarding their effect on psychological well-being, healthy behaviors, and perception of workplace support. Therefore, this study aimed to evaluate the effect of a structured staff wellness program on nurses’ psychological distress, healthy behaviors, and perception of supporting healthy behaviors in a tertiary healthcare setting within the Riyadh Second Healthcare Cluster.
Occupational Stress and Nurse Burnout
Existing evidence indicates that high workload, emotional exhaustion, and prolonged occupational stress significantly contribute to nurse burnout, reduced job satisfaction, and compromised patient care quality, ultimately affecting retention and healthcare system performance (AlMuzaini et al., 2024; Batran, 2019). These challenges remain prevalent, particularly in demanding clinical environments where nurses face sustained workload pressures and emotional demands (Alhassani et al., 2024; Tomaszewska et al., 2024).
Effectiveness of Workplace Wellness Interventions
Workplace wellness interventions, including mindfulness training, resilience programs, and multidisciplinary approaches, have demonstrated effectiveness in improving stress management, mental health outcomes, and engagement in health-promoting behaviors (Patrician et al., 2025). In addition, such programs have been shown to enhance lifestyle practices, including physical activity, nutrition, and sleep quality (Guillaumie et al., 2017).
Wellness interventions incorporating mindfulness training, resilience-building strategies, and recreational or therapeutic activities have also been shown to significantly enhance stress management and promote psychological well-being among healthcare professionals (Alharbi & McKenna, 2025; Cohen, 2023).
Barriers to Participation in Wellness Programs
Despite their benefits, participation in wellness programs is often influenced by organizational and psychosocial barriers, such as heavy workload, staffing shortages, and lack of supportive workplace culture (Browne et al., 2024; Barbosa & de Oliveira, 2025). Emerging evidence suggests that digital and hybrid wellness models may improve accessibility and participation among healthcare professionals (Tyagi et al., 2025; Afshin et al., 2026).
Psychosocial Work Environment and Nurse Well-being
Nurses’ well-being is strongly influenced by psychosocial work conditions, including job demands, autonomy, leadership support, and workplace relationships (Al-Homayan et al., 2023; Nagórska et al., 2026). Conversely, negative workplace factors such as bullying, high workload, and emotional demands further exacerbate stress, burnout, and reduced performance (Azhar et al., 2025; Aiken et al., 2018).
Gaps in Evidence and Saudi Healthcare Context
Although staff wellness programs are increasingly recognized as essential for improving workforce well-being, engagement, and patient care quality (Seaverson, 2025; Levskaya, 2026), evidence regarding their effectiveness, sustainability, and cost-effectiveness remains limited, particularly in Saudi healthcare settings (Shiri et al., 2023).
Existing studies are often single-center and provide limited insight into nurses’ perceptions of organizational support for healthy behaviors, especially in post-pandemic healthcare environments. Additionally, economic pressures and workforce constraints continue to influence the implementation and sustainability of wellness initiatives (Hossny et al., 2026).
Study Rationale
Therefore, this study addresses this gap by evaluating the impact of a structured staff wellness program on nurses’ psychological well-being, healthy behaviors, and perception of workplace support within the Riyadh Second Healthcare Cluster (R2).
METHODOLOGY
Research Setting
The study was conducted within the Riyadh Second Healthcare Cluster (R2), Kingdom of Saudi Arabia, administered by King Fahad Medical City (KFMC). The cluster comprises 12 hospitals and specialty healthcare facilities providing primary, secondary, and tertiary care (Jaber et al., 2025). Due to renovations at the KFMC auditorium, the Staff Wellness Program intervention was held at Prince Mohammed Bin Abdulaziz Hospital (PIMAH), accommodating up to 260 participants. This venue provided a representative environment for registered nurses across the R2 facilities (BayCare Health System, 2025).
Research Design
A quantitative pre-test post-test design was employed to evaluate the effectiveness of the staff wellness program on nurses’ psychological well-being, healthy behaviors, and perception of workplace support.
Study Population and Sample
The study population consisted of registered nurses employed in the 12 hospitals of the R2 cluster. To ensure adequate statistical power for detecting meaningful intervention effects, a sample size of 250 participants was calculated, providing at least 80% power at a 95% confidence level with a 5% margin of error. The calculation also accounted for potential non-response or incomplete data (Charan & Biswas, 2013; Osborne, 2012).
Sampling Technique
A purposive sampling method was employed to select participants from various R2 healthcare facilities. Participation was voluntary and confirmed through electronic consent after official invitations were distributed to all R2 facilities (Etikan et al., 2016).
Criteria of the Study
Inclusion Criteria: Registered nurses, shift managers, unit managers, nurse managers, directors, and quality nurses working in R2 acute or critical care settings (Alharbi & McKenna, 2025). Both Saudi nationals and expatriate nurses were included to reflect workforce diversity.
Exclusion Criteria: Nurses with less than six months of experience, those in non-clinical roles, individuals without a BSN or equivalent, and those with documented neurological or psychiatric conditions that could influence study outcomes. Nurses working outside R2 acute or critical care settings were excluded.
Interventions of the Study
The Staff Wellness Program was a one-day structured intervention aimed at enhancing nurses’ mental health, emotional well-being, and adoption of healthy lifestyle behaviors. It incorporated evidence-based wellness strategies delivered through interactive sessions, followed by a three- month follow-up period to evaluate sustained behavioral change. The intervention took place with five major components: life coaching, art therapy, spa activities, entertainment sessions, and a psychology session.
Life Coaching: Life coaching sessions, led by an experienced stress management and preventive health coach, focused on strategies for reducing stress through physical activity, balanced nutrition, healthy habits, coping skills, and fostering a supportive workplace. The principal investigator coordinated a preparatory virtual meeting with the coach to align the session topics with the research objectives and questionnaire.
Art Therapy: Certified art therapists from King Fahad Medical City (KFMC) led structured workshops encouraging creative expression as a tool for stress relief and emotional regulation. All art materials were prepared in advance by the research team to ensure smooth implementation.
Spa Activities: Professional therapists from Beauty Care provided spa treatments, including massages to promote relaxation, reduce tension, and support psychological well-being. Participants
also received information on maintaining regular self-care practices and were encouraged to continue these wellness strategies beyond the intervention day.
Entertainment Sessions: Recreational activities were coordinated by leaders from the National Neuroscience Institute (NNI), Unit-Based Council (UBC), and Hospital-Based Council (HBC). These sessions included light music, group games, quizzes, and interactive exercises aimed at fostering team spirit, reducing stress, and encouraging positive peer interaction.
Psychology Session: A mental health session was delivered by a specialist from the KFMC Psychology Department. The session focused on emotional well-being, coping mechanisms, and building psychological resilience. The PI ensured all logistical and preparatory arrangements were completed before the session.
Data Collection
The data collection tool was systematically developed and validated for clarity, reliability, and psychometric soundness. It comprised three main sections:
Section 1: Demographic and personal information such as age, gender, marital status, number of children, educational qualification, family status, residential area, nationality, professional role, work schedule, and years of professional experience.
Section 2: The General Health Questionnaire-12 (GHQ-12), developed by Goldberg and Williams (1988), is a standardized, widely used instrument designed to assess psychological distress in general and clinical populations. The questionnaire was originally developed through rigorous psychometric testing, including item selection, factor analysis, and validation against clinical assessments of mental health. Its reliability and validity have been confirmed across multiple populations and settings, including healthcare professionals.
The GHQ-12 comprises 12 items assessing mental health severity over recent weeks, scored on a 4-point Likert scale (0–3), with positive items reverse-scored. Total scores range from 0 to 36, with higher scores indicating greater psychological distress. The 4-point scale was selected to provide sensitivity in detecting varying levels of distress and to align with the study’s objective of evaluating changes in nurses’ mental well-being before and after the Staff Wellness Program.
Section 3: Nurses’ perceptions of supporting healthy behaviors were measured using a structured questionnaire adapted from multiple validated instruments (Tennant et al., 2007). The questionnaire was designed to capture four key domains related to healthy behaviors and workplace support. Although the items were adapted from validated sources, content validation was performed specifically for this study. Five nursing professionals with expertise in clinical practice and research evaluated the questionnaire for clarity, relevance, comprehensiveness, and alignment with the study objectives (Cohen et al., 1997; Moos, 1994; Caplan et al., 1975).
Their feedback was incorporated to refine item wording and structure, ensuring that the tool appropriately measured nurses’ perceptions of supporting healthy behaviors in the R2 hospital context. The questionnaire used a Likert-type rating scale, where higher scores indicated stronger agreement with statements, reflecting better mental health, adoption of healthy behaviors, or perception of a supportive work environment. This scale was chosen to provide sensitivity to detect changes in perceptions before and after the Staff Wellness Program, aligning directly with the study’s objective of evaluating program effectiveness.
Data Collection Procedure
Formal invitations were sent to all 12 hospitals in the R2 cluster, and participation was voluntary. Due to renovations at the KFMC auditorium, both the baseline data collection and the Staff Wellness Program were conducted at PIMAH during a scheduled staff wellness day. Post- intervention data were collected three months later via an electronic survey sent to participants who completed the baseline assessment. This interval allowed participants sufficient time to implement the strategies introduced during the program while maintaining compliance and accuracy of responses. Surveys were completed at two time points, baseline and three months post-intervention, each taking approximately 10 minutes. All completed questionnaires were securely transmitted to the principal investigator to ensure accuracy and minimize bias. Participation was voluntary, and written informed consent was obtained electronically from all participants. Participants were informed about the study purpose, procedures, and their right to withdraw at any time without any impact on their employment or professional responsibilities.
Confidentiality and anonymity were strictly maintained by coding all data and removing personal identifiers. Data were securely stored and accessed only by the research team, and findings were reported in aggregate form to ensure participant privacy.
Data Analysis
Data was analyzed using IBM SPSS Statistics version 25. Categorical variables were summarized as frequencies and percentages, while continuous variables were presented as mean ± standard deviation. Normality was assessed using the Kolmogorov–Smirnov test, which indicated that GHQ-12 (p = 0.12) and healthy behavior scores (p = 0.08) were approximately normally distributed, supporting the use of parametric tests. Paired t-tests were used to compare pre- and post-intervention continuous variables, while the extended McNemar test was applied for categorical data. Pearson correlation analysis assessed the relationship between psychological distress and healthy behaviors. Chi-square tests were used to examine associations between demographic variables and outcomes. Reliability of the instruments was high, with Cronbach’s alpha values of 0.83 (GHQ-12) and 0.89 (Healthy Behavior Tool), and strong test–retest reliability (ICC = 0.81 and 0.86). Statistical significance was set at p < 0.05.
Ethical Consideration
This study received ethical approval from the Institutional Review Board (IRB) of King Fahad Medical City (KFMC), Riyadh, Saudi Arabia with reference number 25-297 on 27th May 2025, prior to the initiation of the staff wellness program and the commencement of data collection. The study was conducted in accordance with the Declaration of Helsinki and KFMC ethical research policies.
RESULTS
Demographic and Personal Information
The study included 250 nurses, and their demographic and professional characteristics are summarized in Table 1. Most participants were female (82.4%) and married (54%). Nearly half had no children (49.6%), while 38.8% had 1–2 children. The predominant age group was 31–40 years (42%). Most participants held a bachelor’s degree (64.4%), and 65.6% were non-Saudi nationals. Professionally, 59.2% were registered nurses, and 68.4% worked more than 8 hours per day.
Table 1: Demographic Variables (n=250)
Demographic variables
Number of nurses
%
Age
20-30 years
75
30.00%
31-40 years
105
42.00%
>40 years
70
28.00%
Gender
Male
44
17.60%
Female
206
82.40%
Marital Status
Single
113
45.20%
Married
135
54.00%
Others
2
0.80%
Number of children
Not applicable
124
49.60%
1 -2 children
97
38.80%
>2 children
29
11.60%
Educational Qualification
Diploma
89
35.60%
Bachelor’s degree
161
64.40%
Higher Education
0
0.00%
Residential Area
Inside the Hospital Campus
129
51.60%
Outside the Hospital
121
48.40%
Family Status
Single
109
43.60%
Living with Family
141
56.40%
Nationality
Saudi
86
34.40%
Non-Saudi
164
65.60%
Professional Role
Registered Nurse
148
59.20%
Shift Manager
26
10.40%
Unit Manager
42
16.80%
Others
34
13.60%
Work Schedule
8 hours per day
79
31.60%
More than 8 hours per day
171
68.40%
Years of Professional Experience
Less than 5 years
107
42.80%
5-10 years
80
32.00%
More than 10 years
63
25.20%
Note: Percentages may not total 100 due to rounding.
Psychological Distress (GHQ-12 Score)
Table 2 presents the comparison of GHQ-12 scores (range: 0–36; higher scores indicate greater psychological distress) before and after the intervention. There was a significant reduction in mean GHQ-12 scores from 17.28 ± 3.39 (pre-test) to 13.40 ± 3.19 (post-test). The mean reduction of 3.88 points (22.45%) indicates a meaningful improvement in psychological well-being.
Table 2: Pre- and Post-Intervention GHQ-12 scores
Domain
Pre-test Mean
± SD
Post-test Mean ± SD
Mean Difference
% of reduction
p-value
GHQ Total (0-36)
17.28 ± 3.39
13.40 ± 3.19
-3.88
22.45 % ↓
<0.001***
Note: GHQ-12 score range: 0–36, Higher scores indicate greater psychological distress ↓ indicates reduction (improvement); ***p < 0.001 indicates statistically significant difference
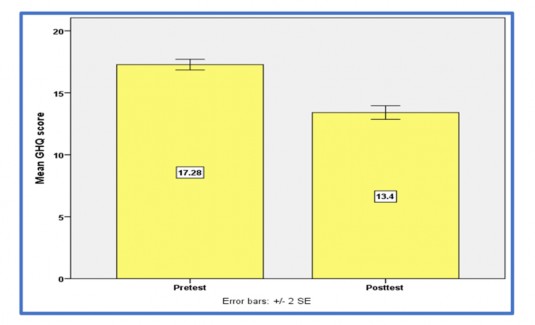
Figure 1: Bar Chart Showing Pre-Test and Post-test GHQ Level
Note: Figure 1 GHQ-12 = General Health Questionnaire (12-item scale; score range: 0–36); Higher scores indicate greater psychological distress, Error bars represent ±2 standard errors (SE); A decrease in scores indicates improvement in psychological well-being; Pretest = baseline assessment; Posttest = assessment after intervention
Healthy Behavior Scores
Table 3 shows the comparison of healthy behavior scores before and after the intervention. The mean score increased from 56.32 ± 8.45 to 65.46 ± 7.92, representing a 16.22% improvement.
Table 3: Pre- and Post-Intervention Healthy Behavior Scores
Domain
Pre-test Mean ±SD
Post-test Mean ± SD
Mean Difference
% of reduction
p-value
Healthy Behavior Score
56.32 ± 8.45
65.46 ± 7.92
9.14
16.22% ↑
<0.001***
Note: Higher scores indicate better engagement in healthy behaviors ↑ indicates improvement; ***p < 0.001 indicates statistically significant difference
Behavioral Domains
All behavioral domains showed statistically significant improvements (Table 4). Stress and coping showed the greatest improvement (27.97%), Overall behavior improved by 19.53%, Workplace support improved by 15.79%
Table 4: Changes in Behavioral Domains
Domain
Pre-test Mean ± SD
Post-test Mean
± SD
Mean Difference
% Gain
p-value
Overall Behavior (0–80)
46.80 ± 9.04
55.94 ± 8.66
9.14
19.53% ↑
<0.001***
General Healthy behaviors
12.70 ± 3.87
13.62 ± 3.14
0.92
7.24% ↑
<0.001***
Stress and Coping
11.94 ± 3.58
15.28 ± 3.64
3.34
27.97% ↑
<0.001***
Workplace Support and Environment
11.90 ± 2.90
13.78 ± 3.23
1.88
15.79% ↑
<0.001***
Note: Higher scores indicate better outcomes, ↑ indicates improvement, ***p < 0.001 indicates statistically significant difference
Perception of Supporting Healthy Behaviors
A statistically significant improvement in perception levels was observed (Table 5). Moderate perception decreased (79.2% → 60.4%) Low perception decreased (20.8% → 6.8%) Very high perception increased (0% → 32.8%)
Table 5: Pre -test and post-test Level of Perception
Level
Pre-test n (%)
Post-test n (%)
Mc Nemar χ²
p-value
Very low
0
0
96.15
0.001***
Low
52 (20.8)
17 (6.8)
Moderate
198 (79.2)
151 (60.4)
Very high
0
82 32.8)
Note: Higher category indicates better perception of workplace support; ***p < 0.001 indicates statistically significant change
Correlation Between Distress and Healthy Behavior
Post-intervention analysis showed a significant negative correlation between psychological distress and healthy behavior (r = −0.37, p = 0.01).

Note: Negative correlation indicates higher distress → lower healthy behavior
Figure 2: Illustrates the correlation between post-test distress scores and healthy behavior scores among nurses.
GHQ-12 = General Health Questionnaire (score range: 0–36), where higher scores indicate greater psychological distress. Each point represents an individual participant, and the fitted line indicates the linear regression trend. The analysis showed a significant inverse relationship between psychological distress and healthy behavior scores (r = −0.37, p = 0.01), indicating that higher distress is associated with lower engagement in healthy behaviors.
DISCUSSION
The present study demonstrated that the staff wellness program had a significant positive impact on nurses’ psychological well-being, healthy behaviors, and perception of workplace support. The findings provide strong evidence that structured wellness interventions can effectively address both the psychological and behavioral dimensions of nurse well-being within a clinical setting.
Psychological Well-Being
A key finding was the significant reduction in psychological distress, as reflected by the decrease in GHQ-12 scores following the intervention. This indicates that the program was effective in improving nurses’ mental health status. The reduction in distress may be attributed to components of the intervention such as stress management strategies, increased awareness, and supportive workplace practices.
These findings are consistent with previous research. Pelissier et al. (2021) reported that workplace wellness programs significantly reduce perceived stress and enhance emotional well-being among nurses. Similarly, Blake et al. (2020) found that mindfulness-based interventions contribute to significant reductions in stress levels. The improvement observed in this study reinforces the importance of integrating mental health support into workplace wellness initiatives. Improved psychological well-being among nurses is particularly important, as it is closely linked to enhanced job performance, reduced absenteeism, and improved patient safety and quality of care.
Healthy Behaviors
The study also revealed a significant improvement in healthy behavior scores, indicating increased adoption of positive lifestyle practices among participants. The overall improvement of 16.22% suggests that the intervention was effective in promoting health-enhancing behaviors despite the challenges of demanding work environments.
All behavioral domains showed statistically significant improvement, with the greatest change observed in stress and coping. This suggests that the program was particularly effective in equipping nurses with practical strategies to manage occupational stress. Improvements in general health behaviors and workplace support further indicate a comprehensive impact of the intervention.
These findings align with Vivarelli and Fenga (2018), who reported that workplace health promotion programs enhance engagement in physical activity, stress management, and self-care. Similarly, Guillaumie et al. (2017) highlighted that nurse wellness programs improve lifestyle behaviors, including nutrition, physical activity, and sleep quality. However, the relatively smaller improvement in general healthy behaviors suggests that sustained and long-term interventions may be required to achieve more substantial behavioral changes.
Perception of Supporting Healthy Behaviors
A notable outcome of this study was the significant shift in nurses’ perception of workplace support, with a marked increase in the “very high” perception category and a reduction in “low” perception levels. This indicates that the wellness program not only influenced individual behaviors but also positively changed how nurses perceived organizational support.
Perception of support plays a critical role in determining engagement in health-promoting activities. When nurses perceive their work environment as supportive, they are more likely to adopt and maintain healthy behaviors. This finding underscores the importance of organizational commitment and leadership involvement in the success of wellness initiatives.
Relationship Between Psychological Distress and Healthy Behaviors
The study identified a significant inverse relationship between psychological distress and healthy behaviors, indicating that nurses who engaged more in healthy practices experienced lower levels of distress. This highlights the interconnected nature of mental health and lifestyle behaviors.
This finding is consistent with Shawon et al. (2023), who reported that healthcare workers engaging in self-care activities exhibited lower levels of stress and burnout. It also supports Pender’s Health Promotion Model, which emphasizes that health-promoting behaviors enhance psychological well- being and resilience.
Additionally, age was the only demographic variable significantly associated with post- intervention distress, suggesting that individual characteristics may influence responsiveness to wellness interventions. This aligns with Shapiro et al. (2019), who found that personal and social factors can affect the effectiveness of wellness programs.
Strengths of the Study
This study has several notable strengths. The use of validated instruments, including the GHQ-12 and the Perception of Supporting Healthy Behaviors Tool, ensured reliable measurement of key variables, with high internal consistency (Cronbach’s alpha = 0.83 and 0.89). The pre-test post-test design enabled the assessment of changes within the same participants, providing valuable insights into intervention effectiveness.
Furthermore, the study was conducted in a real-world clinical setting, enhancing the practical applicability of the findings. The use of robust statistical analyses, including paired t-tests, McNemar’s test, and correlation analysis, further strengthens the validity of the results.
Limitations
Despite these strengths, certain limitations should be acknowledged. The absence of a control group limits the ability to establish causality. The study was conducted within a single healthcare cluster, which may restrict the generalizability of the findings. Additionally, the use of self-reported measures may introduce response bias. The findings highlight the importance of implementing structured staff wellness programs as part of organizational strategies to promote nurse well-being. Healthcare institutions should prioritize mental health support, encourage healthy lifestyle behaviors, and foster supportive work environments.
Future Scope
Future research should employ randomized controlled designs to strengthen causal inference and explore the long-term sustainability of intervention effects. Additionally, examining the impact of nurse wellness on patient outcomes would provide a more comprehensive understanding of the benefits of such programs.
CONCLUSION
The structured staff wellness program demonstrated a significant positive impact on nurses’ psychological well-being, healthy behaviors, and perception of workplace support in the R2 healthcare setting. The reduction in psychological distress alongside improved engagement in health-promoting behaviors indicates that targeted wellness interventions can effectively strengthen nurses’ mental health and lifestyle practices. In addition, the improvement in perception of organizational support highlights the role of workplace wellness initiatives in fostering a more supportive and health-oriented work environment.
Overall, enhancing nurse well-being through structured wellness programs is likely to improve work performance, reduce burnout, and indirectly contribute to safer and higher-quality patient care outcomes. These findings support the integration of sustainable, evidence-based wellness
strategies within healthcare organizations to strengthen both workforce well-being and patient care quality.
Recommendations
Hospitals should routinely implement structured staff wellness programs to reduce psychological distress and encourage healthy behaviors among nurses. Future research should include larger, more diverse samples across multiple regions to enhance generalizability. Longitudinal research is also recommended to evaluate the long-term sustainability of wellness program effects. Integrating wellness initiatives with organizational support, counseling services, and workload management may further enhance outcomes. Finally, personalized wellness strategies should be considered, as demographic factors such as age, residence, and family status were associated with behavioral outcomes.
CRediT Authorship Contribution Statement
P.L.J.C - Conceived and designed the study, Data collection, Data Interpretation, performed analysis, drafted the manuscript. A.A.R - Assisted in study design, supervised data collection, supported data interpretation, critically reviewed the manuscript and final approval.
AI Assistance Declaration
During the preparation of this manuscript, no generative AI tools were used for language enhancement or grammar correction. Generative AI tools were used only for assistance in the preliminary review of literature. All information obtained was critically evaluated, verified, and appropriately cited by the authors. The authors have thoroughly reviewed and revised the manuscript and take full responsibility for the accuracy, originality, and integrity of the final version.
Conflict of Interest
The authors declare that they have no competing interests.
ACKNOWLEDGMENT
The authors sincerely thank the hospital administration of the Riyadh Second Healthcare Cluster (R2) and King Fahad Medical City for granting permission and providing institutional support to conduct this study. The authors also acknowledge the National Neuroscience Institute staff, Unit- Based Council (UBC), and Hospital-Based Council (HBC) members for their assistance in organizing the Staff Wellness Program. Special appreciation is extended to all nurses who voluntarily participated in the study and contributed their time and valuable responses.
REFERENCES
Afshin, P., Mutonyi, B. R., & Nybakk, E. (2026). Digital job demands and healthcare workers' workplace well-being: the mediating role of job and personal resources. Frontiers in Health Services, 6, 1743364. https://doi.org/10.3389/frhs.2026.1743364
Aiken, L. H., Ceron, C., Simonetti, M., Lake, E. T., Galiano, A., Garbarini, A., ... & Smith, H. L. (2018). Hospital nurse staffing and patient outcomes. Revista Médica Clínica Las Condes, 29(3), 322-327. https://doi.org/10.1016/j.rmclc.2018.04.011
Alharbi, M. S., Albughuli, M. B., Aljohani, S. S., Alraddadi, Y. A., Alalawi, N. B., Alawfi, H. M., Al Harbi, S. M., Alharbi, R. H., & Alreshidi, O. A. (2025). Nurses' well-being and its relationship with quality of nursing work life at Alsalam and Al Haram Hospitals, Saudi Arabia. Frontiers in public health, 13, 1678358. https://doi.org/10.3389/fpubh.2025.1678358
Alharbi, B. A. A., & McKenna, N. (2025). A systematic review of mindfulness-based interventions to reduce ICU nurse burnout: global evidence and thematic synthesis. BMC nursing, 24(1), 927. https://doi.org/10.1186/s12912-025-03507-w
Alhassani, F. K. H., Alzahrani, A. S., Alhassani, H. H. K., Alhazmi, W. S., Dandini, M. T., Alsubhi, M. M., ... & Alhassani, H. K. H. (2024). Occupational Stress and Burnout in Healthcare Workers: Causes, Consequences, And Solutions. Cultura: International Journal of Philosophy of Culture and Axiology, 21(1s), 22-33. https://culturajournal.com/submissions/index.php/ijpca/article/view/1638/1773
Al-Homayan, A. M., Shamsudin, F. M., Subramaniam, C., & Islam, R. (2013). Impacts of Job Demands on Nurses' performance Working in Public Hospitals. American Journal of Applied Sciences, 10(9), 1050. https://doi.org/10.3844/ajassp.2013.1050.1060
AlMuzaini, A. S., AlRasheedi, B. S., AlShahrani, F. F., AlOtaibi, H. B., AlHagan, J. A. M., AlOtaibi, K. R. H., ... & Alanzi, T. S. (2024). Workplace well-being in nursing: a systematic review of trends in burnout, job satisfaction, and retention. Journal of International Crisis and Risk Communication Research, 7(S9), 3103. https://doi.org/10.63278/jicrcr.vi.2174
Azhar, M., Ahmad, D. G., Khan, M., Shaheen, S., Sultan, A., & Bari, F. (2025). “Psychological Perspectives on Workplace Bullying and its Influence on Nursing Performance” A Cross-Sectional Study. TPM–Testing, Psychometrics, Methodology in Applied Psychology, 32(S3 (2025): Posted 07 July), 2510-2516. https://tpmap.org/submission/index.php/tpm/article/view/4156
Barbosa, I., & de Oliveira, E. R. (2025). Beyond image: evaluating the perceived effectiveness of workplace mental health programs in the insurance sector. BMC public health, 25(1), 218. https://doi.org/10.1186/s12889-025-21302-9
Batran, A. (2019). Work related stress among Saudi nurses working in intensive care units. Open Journal of Nursing, 9(11), 1143-1152. https://doi.org/10.4236/ojn.2019.911084
BayCare Health System. (2025, May 12). BayCare expands nurse well-being program systemwide. PR Newswire. https://www.prnewswire.com/news-releases/baycare-expands-nurse-well-being- program-systemwide-302452392.html
Blake, H., Bermingham, F., Johnson, G., & Tabner, A. (2020). Mitigating the psychological impact of COVID-19 on healthcare workers: a digital learning package. International journal of environmental research and public health, 17(9), 2997. https://doi.org/10.3390/ijerph17092997
Browne, J., Penn, D. L., Meyer-Kalos, P., Gottlieb, J. D., & McGurk, S. R. (2024). Factors influencing engagement in in-person and remotely delivered lifestyle interventions for young adults with serious mental illness: A qualitative study. Early Intervention in Psychiatry, 18(1), 42–48. https://doi.org/10.1111/eip.13432
Caplan, R. D., Cobb, S., French, J. R. P., Harrison, R. V., & Pinneau, S. R. (1975). Job demands and worker health: Main effects and occupational differences (Vol. 75). US Department of Health, Education, and Welfare, Public Health Service, Center for Disease Control, National Institute for Occupational Safety and Health. https://ntrl.ntis.gov/NTRL/dashboard/searchResults/titleDetail/PB276809.xhtml
Charan, J., & Biswas, T. (2013). How to calculate sample size for different study designs in medical research? Indian Journal of Psychological Medicine, 35(2), 121–126. https://doi.org/10.4103/0253-7176.116232
Cohen, C., Pignata, S., Bezak, E., Tie, M., & Childs, J. (2023). Workplace interventions to improve well-being and reduce burnout for nurses, physicians and allied healthcare professionals: a systematic review. BMJ open, 13(6), e071203. https://doi.org/10.1136/bmjopen-2022-071203
Cohen, S., Kessler, R. C., & Gordon, L. U. (Eds.). (1997). Measuring stress: A guide for health and social scientists. Oxford University Press. https://onlinelibrary.wiley.com/doi/10.1002/(SICI)1099-1700(199701)13:1%3C67::AID- SMI730%3E3.0.CO;2-8
Etikan, I., Musa, S. A., & Alkassim, R. S. (2016). Comparison of convenience sampling and purposive sampling. American Journal of Theoretical and Applied Statistics, 5(1), 1–4. https://doi.org/10.11648/j.ajtas.20160501.11
Goldberg, D. P., & Williams, P. (1988). A user's guide to the General Health Questionnaire. NFER-Nelson. https://effectiveservices.my.site.com/s/measure/a007R00000v8QVxQAM/general-health- questionnaire
Guillaumie, L., Boiral, O., & Champagne, J. (2017). A mixed‐methods systematic review of the effects of mindfulness on nurses. Journal of advanced nursing, 73(5), 1017-1034. https://doi.org/10.1111/jan.13176
Hossny, E. K., Aly, S. E., Mohamed, I. A., Abdelkader, A. M., Abdelrahem, A. S. A., Mohammed, F. M., Al-Yafeai, T. M., & Younes, H. S. (2026). Nurses’ Perceptions of the Effect of Organizational Support, Role Clarity, and Ambiguity on Career Plateauing: Implications for the Healthcare Workforce. Healthcare, 14(6), 755. https://doi.org/10.3390/healthcare14060755
Hussein, A. H. M., Abou Hashish, E. A., & Younes, B. M. (2024). The Relationship Between Nurses' Psychological Well-Being and Their Work Productivity Loss: A Descriptive Correlational Study. SAGE open nursing, 10, 23779608241285400. https://doi.org/10.1177/23779608241285400
Jaber, M. J., Bindahmsh, A. A., Baker, O. G., Alaqlan, A., Almotairi, S. M., Elmohandis, Z. E., ... & Abuzir, B. M. (2025). Burnout combating strategies, triggers, implications, and self-coping mechanisms among nurses working in Saudi Arabia: a multicenter, mixed methods study. BMC nursing, 24(1), 590. https://doi.org/10.1186/s12912-025-03191-w
Levskaya, L. (2026, February 4). Wellness programs for healthcare professionals. Meditopia. https://meditopia.com/en/forwork/articles/wellness-programs-for-healthcare
Moos, R. H. (1994). Work environment scale manual, Consulting Psychologists Press. https://creativesprague.weebly.com/uploads/6/0/9/1/60910867/_workenvironmentscale.pdf
Nagórska, M., Červený, M., Rękas, M., Lesiak, A., Chmiel, Z., Zamboriová, M., ... & Cruz, J. P. (2026). Nurses’ Perception of the Hospitals’ Spiritual Climate and Its Influence on Their Organizational Commitment: A Cross‐Sectional and Correlational Study. Journal of Nursing Management, 2026(1), 5163550. https://doi.org/10.1155/jonm/5163550
Osborne, J. W. (2012). Best practices in data cleaning: A complete guide to everything you need to do before and after collecting your data. Sage publications, Inc. https://doi.org/10.4135/9781452269948
Patrician, P. A., Stewart, J., Montgomery, A., Morson, D. M., Carter, J. L., Travis, J. R., ... & Beam, T. (2025). Building an Effective Team to Improve Wellness Outcomes Among Nurses: The Critical Role of Leadership. Nurse Leader, 23(3), 277-283. https://doi.org/10.1016/j.mnl.2025.03.008
Pelissier, C., Fort, E., Charbotel, B., & Hours, M. (2021). Factors associated with psychological distress in French medical students during the COVID-19 health crisis. International Journal of Environmental Research and Public Health, 18(24), 12951. https://doi.org/10.3390/ijerph182412951
Seaverson, E. (2025, November 18). 2026 workplace wellness trends you need to know. WebMD Health Services. https://www.webmdhealthservices.com/blog/2026-workplace-wellness-trends- you-need-to-know/
Shawon, M. S. R., Rouf, R. R., Jahan, E., Hossain, F. B., Mahmood, S., Gupta, R. D., ... & Islam, S. (2023). The burden of psychological distress and unhealthy dietary behaviours among 222,401 school-going adolescents from 61 countries. Scientific reports, 13(1), 21894. https://doi.org/10.1038/s41598-023-49500-8
Shapiro, S. L., Brown, K. W., & Biegel, G. M. (2019). Teaching self-care to caregivers: Effects of mindfulness-based stress reduction on the mental health of therapists in training. Training and Education in Professional Psychology, 13(2), 105-115. https://doi.org/ 10.1037/1931-3918.1.2.105
Shiri, R., Nikunlaakso, R., & Laitinen, J. (2023). Effectiveness of Workplace Interventions to Improve Health and Well-Being of Health and Social Service Workers: A Narrative Review of Randomised Controlled Trials. Healthcare, 11(12), 1792. https://doi.org/10.3390/healthcare11121792
Tennant, R., Hiller, L., Fishwick, R., Platt, S., Joseph, S., Weich, S., Parkinson, J., Secker, J., & Stewart-Brown, S. (2007). The Warwick-Edinburgh mental well-being scale (WEMWBS). Health and Quality of Life Outcomes, 5, 63. https://doi.org/10.1186/1477-7525-5-63
Tomaszewska, K., Kowalczuk, K., Kadučáková, H., Lehotská, M., Papp, K., & Majchrowicz, B. (2024). Occurrence of Stress and Burnout Among Nurses Employed in a Psychiatric Hospital and a Somatic Hospital-A Comparative Analysis (Nursing Workload KEGA č. 011KU- 4/2024). Healthcare (Basel, Switzerland), 12(23), 2443. https://doi.org/10.3390/healthcare12232443
Tyagi, S., Mishra, S., & Dey, A. K. (2025). Well-being among health care professionals: A hybrid review, integrative framework, and research agenda. International Journal of Stress Management, 32(1), 47. https://doi.org/10.1037/str0000337
Vivarelli, S., & Fenga, C. (2024). Workplace health promotion program: an integrated intervention to promote well-being among healthcare workers. Public Health Toxicology, 4(3), 1-8. https://doi.org/10.18332/pht/192700
Demographic variables
Number of nurses
%
Age
20-30 years
75
30.00%
31-40 years
105
42.00%
>40 years
70
28.00%
Gender
Male
44
17.60%
Female
206
82.40%
Marital Status
Single
113
45.20%
Married
135
54.00%
Others
2
0.80%
Number of children
Not applicable
124
49.60%
1 -2 children
97
38.80%
>2 children
29
11.60%
Educational Qualification
Diploma
89
35.60%
Bachelor’s degree
161
64.40%
Higher Education
0
0.00%
Residential Area
Inside the Hospital Campus
129
51.60%
Outside the Hospital
121
48.40%
Family Status
Single
109
43.60%
Living with Family
141
56.40%
Nationality
Saudi
86
34.40%
Non-Saudi
164
65.60%
Professional Role
Registered Nurse
148
59.20%
Shift Manager
26
10.40%
Unit Manager
42
16.80%
Others
34
13.60%
Work Schedule
8 hours per day
79
31.60%
More than 8 hours per day
171
68.40%
Years of Professional Experience
Less than 5 years
107
42.80%
5-10 years
80
32.00%
More than 10 years
63
25.20%
Domain
Pre-test Mean
± SD
Post-test Mean ± SD
Mean Difference
% of reduction
p-value
GHQ Total (0-36)
17.28 ± 3.39
13.40 ± 3.19
-3.88
22.45 % ↓
<0.001***
Domain
Pre-test Mean ±SD
Post-test Mean ± SD
Mean Difference
% of reduction
p-value
Healthy Behavior Score
56.32 ± 8.45
65.46 ± 7.92
9.14
16.22% ↑
<0.001***
Domain
Pre-test Mean ± SD
Post-test Mean
± SD
Mean Difference
% Gain
p-value
Overall Behavior (0–80)
46.80 ± 9.04
55.94 ± 8.66
9.14
19.53% ↑
<0.001***
General Healthy behaviors
12.70 ± 3.87
13.62 ± 3.14
0.92
7.24% ↑
<0.001***
Stress and Coping
11.94 ± 3.58
15.28 ± 3.64
3.34
27.97% ↑
<0.001***
Workplace Support and Environment
11.90 ± 2.90
13.78 ± 3.23
1.88
15.79% ↑
<0.001***
Level
Pre-test n (%)
Post-test n (%)
Mc Nemar χ²
p-value
Very low
0
0
96.15
0.001***
Low
52 (20.8)
17 (6.8)
Moderate
198 (79.2)
151 (60.4)
Very high
0
82 32.8)