Original Article
Development and Pilot Evaluation of a Self-Guided Digital Hypnorelaxation Program for Sleep Quality and Psychological Readiness Pregnant Women
Nurul Jannah*, Gunavathy Selvarajh
School of Nursing and Applied Science, Lincoln University College, Wisma Lincoln, No. 12-18, Jalan SS 6/12, 47301 Petaling Jaya, Selangor Darul Ehsan, Malaysia
*Corresponding Author’s Email: jannah.phdscholar@lincoln.edu.my
Abstract
Background: Sleep disturbances and psychological distress are common during late pregnancy and are associated with reduced maternal well-being and childbirth preparedness, highlighting the need for accessible non-pharmacological interventions. Objectives: This pilot study aimed to develop and preliminarily evaluate the feasibility and early responsiveness of a self-guided digital hypnorelaxation program integrating relaxation techniques and positive affirmations for late pregnancy. Methods: A developmental quasi-experimental pilot study with a pretest–posttest comparison group design was conducted among 60 third-trimester pregnant women recruited from community antenatal care settings. Participants were non-randomly allocated to an intervention group (n = 35) and a routine care group (n = 25). The intervention consisted of a standardized hypnorelaxation audio program used independently twice daily for 14 days. Sleep-related well-being and psychological readiness for childbirth were assessed using validated Indonesian instruments and analyzed within an exploratory pilot framework. Results: Baseline characteristics were comparable between groups. The intervention group showed greater short-term changes in sleep-related well-being scores (mean change = 8.40) compared with minimal change in the control group (mean change = 0.30). A shift toward higher sleep quality categories and increased childbirth preparedness was observed, with 85.7% of participants classified as highly prepared post-intervention. These findings represent preliminary response patterns within a pilot context. Conclusion: The intervention demonstrated feasibility, high adherence, and early indications of responsiveness. Further randomized controlled trials are required to establish effectiveness.Keywords: Digital Hypnorelaxation; Late Pregnancy; Maternal Well-Being; Pilot Study; Sleep Quality
Introduction
Pregnancy is characterized by profound physiological, psychological, and social adaptations that intensify during late gestation, a period when sleep disturbances and emotional strain become increasingly prevalent. Hormonal changes, progressive fetal growth, and physical discomfort including musculoskeletal pain, nocturnal urination, and difficulty maintaining restful positions substantially contribute to deteriorating sleep quality and heightened psychological distress among pregnant women (Abera et al., 2024; Özkan & Rathfisch, 2018; Sanlı et al., 2022). Accumulating evidence indicates that poor sleep quality and elevated psychological distress during late pregnancy are not only sources of maternal discomfort but are also associated with adverse obstetric and neonatal outcomes, including hypertensive disorders, antenatal mood disturbances, preterm birth, and increased obstetric interventions (Abera et al., 2024; Paulino et al., 2022; Werner et al., 2020).
Pharmacological options for managing sleep and emotional difficulties during pregnancy remain constrained by fetal safety considerations, thereby increasing reliance on non-pharmacological strategies within antenatal care. Mind body interventions such as guided relaxation, hypnosis-based techniques, breathing exercises, and cognitive emotional regulation approaches have demonstrated beneficial effects on sleep quality and psychological well-being during pregnancy (Nasiri et al., 2018; Catsaros & Wendland, 2020; Wang et al., 2025; Afriyanti et al., 2021; Eliyawati, 2024). Hypnosis- oriented relaxation facilitates autonomic nervous system regulation and focused attention, while positive affirmations enhance self-efficacy and emotional coping capacities mechanisms particularly relevant during late pregnancy when vulnerability to stress and fatigue is heightened (Fernández et al., 2024; Vázquez-Lara et al., 2025;). From a biopsychophysiological perspective, these approaches are understood to modulate autonomic balance, reduce cognitive hyperarousal, and strengthen adaptive cognitive emotional processing, which are key pathways influencing sleep and psychological readiness during pregnancy. Integrating these complementary components may generate synergistic benefits beyond those achieved through single-modality interventions alone (Catsaros & Wendland, 2020; Manesh et al., 2023).
Advances in digital health delivery have created new opportunities for translating relaxation-based interventions into accessible, self-guided formats that can be used independently by pregnant women within routine care environments. Audio-based digital interventions, in particular, offer scalable and low- resource approaches that reduce reliance on direct provider supervision while maintaining therapeutic structure (Downe et al., 2015; Li et al., 2025). However, despite growing evidence supporting hypnosis and relaxation techniques, most existing interventions remain provider-dependent, group-based, or require structured supervision, limiting scalability and real-world implementation in routine antenatal care, particularly in low-resource settings. Limited research has systematically developed, and pilot- tested integrated, self-guided digital relaxation programs specifically tailored to the needs of women in late pregnancy. Moreover, previous studies have rarely combined multiple mechanisms such as physiological relaxation, cognitive reframing, and affirmation-based self-regulation within a single standardized digital intervention framework. Most existing studies have focused on face-to-face, group- based, or provider-led interventions, leaving a notable gap in evidence regarding feasible, independently usable digital solutions for maternal well-being, especially in community and resource- limited settings (Fernández et al., 2024; Paulino et al., 2022; Akinwaare & Oluwatosin, 2023).
To address this gap, the present pilot study aimed to systematically develop and preliminarily evaluate a self-guided digital hypnorelaxation program integrating guided relaxation and positive affirmations for women in late pregnancy. This study is novel in that it introduces an integrated, standardized, and fully self-guided digital intervention model designed for independent use within routine antenatal care settings. Consistent with a developmental pilot framework, the study emphasizes feasibility, adherence, and early response patterns rather than causal effectiveness. By explicitly positioning the intervention within a biopsychosocial regulatory framework and evaluating its early responsiveness in real-world settings, this research contributes foundational evidence to support future refinement and randomized evaluation of scalable non-pharmacological interventions within antenatal care systems.
Methodology Study Design
This study employed a developmental pilot design using a quasi-experimental pretest–posttest comparison group framework to support the systematic development and preliminary evaluation of a self-guided digital hypnorelaxation intervention. The primary objectives were to assess feasibility, adherence, and early response patterns rather than to establish causal effectiveness or clinical efficacy. This approach aligns with early-phase digital health intervention research intended to inform subsequent rigorously designed randomized controlled trials.
A pragmatic partial randomization approach was applied. At the cluster level, primary health care centers (Puskesmas) were selected to represent routine antenatal care settings within the study area. Within each site, eligible participants were recruited consecutively and allocated using a structured recruitment process incorporating elements of random selection. Full individual randomization was not implemented due to logistical and ethical constraints in community-based antenatal care settings. Participants in both groups were recruited concurrently during the same study period to minimize temporal bias. Although formal matching procedures were not applied, baseline comparability between groups was assessed to partially address potential selection bias, which is acknowledged as a limitation of this pilot study.
Study Setting and Participants
The study was conducted in community-based antenatal care settings within the service area of the Semarang District Health Office, Central Java, Indonesia, between May and August 2025. Third- trimester pregnant women (28–36 weeks of gestation) were purposively recruited from primary health care centers (Puskesmas) during routine antenatal visits. Eligibility criteria included singleton pregnancy, absence of major obstetric complications, no current use of sedative or sleep-related medications, and provision of informed consent. Women with high-risk pregnancies or diagnosed psychiatric disorders were excluded. A total of 70 eligible participants were initially enrolled and allocated into the intervention group (n = 35) and the control group (n = 35) as part of this developmental pilot study.
The initial sample size was determined based on contemporary methodological guidance for pilot and feasibility studies, which prioritizes feasibility assessment and parameter estimation rather than formal hypothesis testing. Recent evidence suggests that sample sizes of approximately 20–50 participants per group are sufficient to obtain stable estimates, with around 30 participants per arm commonly used to inform future definitive trials (Teresi et al., 2022; Totton et al., 2023; Montgomery, 2025). Accordingly, the planned sample size (n = 70) was considered adequate and consistent with these methodological recommendations. During the 14-day follow-up period, 10 participants in the control group did not complete the post-intervention assessment due to loss to follow-up and scheduling constraints related to routine antenatal visits, while no dropouts were observed in the intervention group.
Consequently, the final analytic sample consisted of 60 participants, including 35 in the intervention group and 25 in the control group. This final sample size remains within the acceptable range for pilot studies and is considered sufficient to evaluate feasibility, adherence, and preliminary response patterns in early-phase intervention research. Complete case analysis was applied in accordance with the exploration nature of the study.
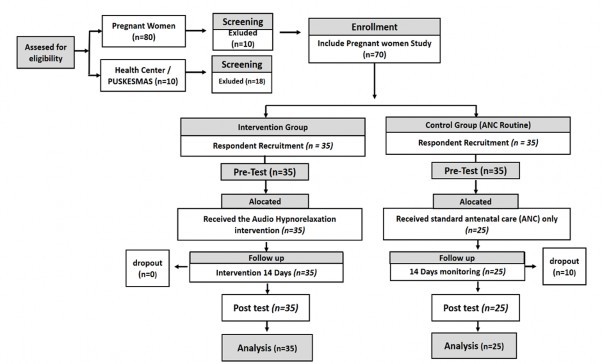
Figure 1: CONSORT Flow Diagram of Participant Recruitment and Retention in the Pilot Study
Development of the Audio-Based Relaxation Program (Expert- and Technology-Validated)
The digital hypnorelaxation program was systematically developed following a structured developmental framework for maternal digital health interventions and grounded in empirical evidence from relaxation-based, hypnosis-oriented, and affirmation-focused approaches. The development process involved a multidisciplinary expert panel consisting of midwifery academics (lecturers with expertise in maternal health), experienced clinical midwives, and information technology (IT) specialists to ensure clinical relevance, theoretical rigor, and technical usability of the intervention. Midwifery experts contributed to clinical appropriateness, maternal health relevance, and contextual adaptation of the content, while IT specialists evaluated the digital delivery format, user accessibility, and audio usability to ensure the intervention was feasible for independent use in real-world settings.
The intervention was standardized and delivered as a 20-minute audio session consisting of four sequential components: (1) diaphragmatic breathing (3–5 minutes) to initiate physiological relaxation; (2) progressive muscle relaxation (5–7 minutes) targeting major muscle groups; (3) guided hypnotic relaxation and imagery (5–7 minutes) to enhance focused attention and autonomic regulation; and (4) positive affirmations (3–5 minutes) to reinforce emotional safety, self-efficacy, and childbirth preparedness. Content validity, clinical appropriateness, and usability were evaluated through expert review, resulting in an overall content validity index (CVI) of 0.90, indicating high relevance, clarity, and applicability of the intervention components. The program was refined iteratively based on expert feedback and finalized as an evidence-informed, context-adapted digital intervention suitable for self- guided use within routine antenatal care settings.
Intervention Procedures
Baseline assessments (pre-test) were conducted on Day 0 using validated instruments. Participants in the intervention group received standardized instructions for independent use of the self-guided digital hypnorelaxation program. The intervention was delivered as a standardized, pre-recorded digital audio program designed for self-guided use. The audio content was recorded using a standard digital voice recording system to ensure clarity, consistency, and appropriate sound quality. The narration was delivered using a calm and steady tone with controlled pacing to facilitate relaxation. The final audio file was produced in MP3 format and distributed via a commonly used mobile messaging platform, allowing participants to access the program through their personal smartphones without additional applications. Structure of the Audio Session (±20 minutes). This Protocol:
Tabel 1: Intervention Protocol
Phase
Component
Duration
Objective
Example Script
Phase I
Diaphragmatic Breathing
3–5
minutes
Initiate physiological relaxation through controlled breathing
“Now, sit or lie down comfortably… Take a slow breath through your nose… hold briefly… exhale slowly through your mouth… Feel your abdomen rise as you inhale and fall as you exhale… Each breath brings calmness… each exhale releases tension…”
Phase II
Progressive Muscle Relaxation
5–7
minutes
Reduce muscle tension and promote full-body relaxation
“Bring your attention to your body… Start from your feet… release tension… Calves… thighs… abdomen… chest… shoulders… arms… hands… neck… face… Let your entire body feel light, warm, and relaxed…”
Phase III
Guided Hypnotic Relaxation & Imagery
5–7
minutes
Reduce cognitive hyperarousal and enhance mental calmness
“Imagine yourself in a peaceful place… safe and comfortable… Perhaps at the beach or in a quiet garden… Feel a gentle breeze… Your mind becomes calm… All worries drift away… You are safe… You are calm…”
Phase IV
Positive Affirmations
3–5
minutes
Strengthen self- efficacy, emotional calmness, and childbirth readiness
“My body is capable of supporting a healthy pregnancy… I feel calm and relaxed as I prepare for sleep… I trust myself… I am confident and ready for childbirth… I am strong… I am capable… I am ready…”
Closing
Closing Relaxation
±1 menit
Relaxation
“Stay in this calm state… Take a slow breath… When you are ready, gently open your eyes… feeling relaxed, refreshed, and at ease…”
Participants were instructed to listen to the audio twice daily (morning and evening before sleep) for fourteen consecutive days. Adherence was defined as completion of at least 20 of the 28 sessions and was monitored using self-report logs. Only brief initial guidance was provided, and no continuous supervision was implemented, consistent with the self-guided design. The comparison group continued routine antenatal care without additional intervention. Post-intervention assessments were conducted on Day 14 using the same instruments.
Bias Control
Several procedures were implemented to minimize potential sources of bias in this pilot study. First, both intervention and control groups were assessed at identical time points (Day 0 and Day 14) using standardized measurement procedures to ensure consistency. Second, participants were recruited concurrently during the same study period to reduce temporal bias. Third, although blinding was not feasible due to the nature of the intervention, standardized instructions and uniform data collection procedures were applied across groups to reduce measurement bias. To minimize contamination, participants were instructed not to share the intervention audio or engage in additional relaxation practices during the study period. Adherence was monitored using self-reported logs, and although this may introduce reporting bias, it was considered acceptable within the feasibility-oriented framework of this pilot study.
Measurement Instruments
Sleep-related well-being was assessed using the Maternal Sleep Quality Index for the Third Trimester – Indonesian Version an eight-item self-report instrument developed and validated for pregnant women in Indonesia (Jannah & Selvarajh, 2026a). The instrument was administered in Bahasa Indonesia, ensuring linguistic and cultural appropriateness. The scale comprises three dimensions (sleep initiation and continuity, pregnancy-specific disturbance, and daytime impact and fatigue) and demonstrated acceptable construct validity based on Confirmatory Factor Analysis (CFI = 0.95; TLI = 0.93; RMSEA = 0.094; SRMR = 0.027), with strong factor loadings (0.91–0.99, p < .001). Higher scores indicate poorer sleep quality, and scores were categorized as poor, fair, good, and very good levels as presented in Table 4. Psychological readiness for childbirth was measured using the Childbirth Readiness Questionnaire a nine-item instrument validated in Indonesian pregnant populations (Jannah & Selvarajh, 2026b). This instrument was also administered in Bahasa Indonesia. Content validity was acceptable (I-CVI ≥ 0.80), with item–total correlations ranging from 0.34 to 0.61 and internal consistency (α = 0.82). In the present study, reliability was confirmed (MSQI-T3-ID α = 0.89; CRQ α = 0.93). Higher scores indicate greater readiness, and scores were categorized into low, moderate, and high levels as shown in Table 6.
Data Collection and Analysis
Baseline data were collected on Day 0 and follow-up data on Day 14. Data analysis followed an exploratory pilot framework. Normality was assessed prior to inferential testing. Paired and independent t-tests were applied to sleep-related outcomes, while Wilcoxon signed-rank and Mann–Whitney U tests were used for non-parametric data. Given the pilot nature of the study, statistical analyses were intended to describe preliminary response patterns rather than to test definitive hypotheses or establish causal relationships. Emphasis was placed on descriptive trends and early responsiveness. No adjustments for multiple testing were applied, consistent with methodological guidance for pilot studies.
Ethical Consideration
Ethical approval for this study was obtained from the Faculty of Psychology, Diponegoro University, Indonesia with Approval No. 53/UN7.F11/PP/XI/2024; approved on 5th November, 2024.
Results
Participant Characteristics
To provide an overview of the study sample, participant demographic characteristics were examined and compared between the intervention and control groups.Table 2. Demographic Characteristics of Participants
Characteristic
Intervention (n=35)
Control (n=25)
Age (years)
<25
9 (25.7%)
5 (20.0%)
25–35
19 (54.3%)
15 (60.0%)
>35
7 (20.0%)
5 (20.0%)
Gravidity
Primigravida
16 (45.7%)
10 (40.0%)
Multigravida
19 (54.3%)
15 (60.0%)
Occupation
Employed
14 (40.0%)
12 (48.0%)
Homemaker
21 (60.0%)
13 (52.0%)
Education Level
Low
12 (34.3%)
7 (28.0%)
Middle
14 (40.0%)
12 (48.0%)
Higher
9 (25.7%)
6 (24.0%)
Table 2 presents the demographic characteristics of the participants. The intervention and control groups demonstrated broadly comparable profiles across age, gravidity, occupation, and education level. Most participants were aged between 25 and 35 years, and the distribution of key characteristics appeared relatively balanced between groups, supporting baseline comparability for exploration analysis within this pilot study.
Table 3: Adherence to the Audio-Based Relaxation Program (Intervention Group)
Adherence Level
Sessions Completed
n
%
High–Moderate
24–28
30
85.7
Minimum
20–23
5
14.3
Adherence to the audio-based hypnorelaxation program is summarized in Table 3. The majority of participants (85.7%) completed 24–28 sessions, exceeding the predefined adherence threshold, while the remaining participants met the minimum adherence criterion. No discontinuation was observed in the intervention group. These findings indicate good feasibility and acceptability of the self-guided digital intervention during the 14-day implementation period.
Sleep-Related Well-Being
Sleep-related well-being was assessed to describe baseline conditions and short-term changes observed during the study period.
Table 4: Sleep-Related Well-Being Before and After the Study Period
Group
Pre-test Mean ± SD
Post-test Mean ± SD
Mean Change
p-value
Intervention
17.3 ± 2.1
8.9 ± 2.0
8.40
<0.001
Control
17.6 ± 2.3
17.3 ± 2.4
0.30
0.326
As shown in Table 4, baseline sleep-related well-being scores were comparable between groups. Over the 14-day period, the intervention group showed greater changes in sleep quality scores (mean change
= 8.40), whereas the control group demonstrated minimal change (mean change = 0.30). These findings represent short-term response patterns observed within the pilot framework rather than evidence of clinical effectiveness.
Table 5: Distribution of Sleep Quality Categories
Category
Intervention
Control
Pre
Post
Pre
Post
Poor
9 (25.7%)
0 (0%)
8 (32.0%)
8 (32.0%)
Fair
26 (74.3%)
0 (0%)
17 (68.0%)
16 (64.0%)
Good
0 (0%)
30 (85.7%)
0 (0%)
1 (4.0%)
Very good
0 (0%)
5 (14.3%)
0 (0%)
0 (0%)
Table 5 presents the distribution of sleep quality categories before and after the intervention period. In the intervention group, a shift from poor and fair categories at baseline toward good and very good categories was observed following the intervention. In contrast, the distribution in the control group remained largely unchanged over time.This redistribution reflects descriptive changes in sleep quality categories consistent with the exploratory nature of the study.
Psychological Readiness for Childbirth
Psychological readiness for childbirth was evaluated to describe changes in preparedness levels during the study period.
Table 6: Childbirth Preparedness Scores and Category Distribution
Group
Median (IQR)
p-value
Pre-test
Post-test
Intervention
4 (3–5)
12 (11–14)
<0.001
Control
4 (3–5)
5 (4–7)
0.264
As shown in Table 6, baseline preparedness scores were similar between groups. Following the intervention, the intervention group demonstrated higher post-test scores (median = 12), whereas the control group showed only modest changes (median = 5). These findings indicate preliminary changes in preparedness levels and should be interpreted as early response patterns within the pilot design.
Table 7: Distribution of Childbirth Preparedness Categories
Category
Intervention
Control
Pre
Post
Pre
Post
Low
26 (74.3%)
0 (0%)
18 (72.0%)
17 (68.0%)
Moderate
9 (25.7%)
5 (14.3%)
7 (28.0%)
8 (32.0%)
High
0 (0%)
30 (85.7%)
0 (0%)
0 (0%)
Table 7 illustrates the distribution of childbirth preparedness categories. In the intervention group, a marked shift from low to high preparedness categories was observed following the intervention period. In contrast, the control group remained predominantly within low to moderate categories. These categorical changes provide descriptive support for observed trends in psychological readiness, consistent with the feasibility-oriented objectives of the study.
Discussion
Preliminary Sleep Quality Responses to the Self-Guided Digital Hypnorelaxation Program
This developmental pilot study examined early response patterns associated with a self-guided digital hypnorelaxation program designed to support maternal well-being in late pregnancy. Within this exploratory framework, participants who independently engaged with the digital audio intervention showed relatively greater short-term changes in sleep-related well-being compared with those receiving routine antenatal care, despite comparable baseline conditions. Importantly, these findings should be interpreted as preliminary responsiveness rather than evidence of clinical effectiveness, consistent with the objectives of early-phase intervention research. The observed response patterns are broadly consistent with prior evidence indicating that non-pharmacological, relaxation-based strategies may positively influence sleep quality during pregnancy, particularly in the third trimester when physiological discomfort and emotional vulnerability intensify. Systematic reviews and meta-analyses have documented associations between hypnosis-based relaxation, guided imagery, and improved sleep outcomes among pregnant populations (Abera et al., 2024; Paulino et al., 2022; Chamine et al., 2018; Nasiri et al., 2018).
The present study extends this literature by suggesting the feasibility and early responsiveness of a fully self-guided digital delivery format, whereas many previous studies have relied on provider-led, face-to-face, or group-based interventions. This distinction is important, as digital self-guided approaches may have the potential to enhance scalability and accessibility within routine antenatal care settings. Mechanistically, digitally guided hypnorelaxation is hypothesized to facilitate autonomic nervous system regulation through enhanced parasympathetic activation, reduced muscular tension,and attenuation of cognitive hyperarousal that disrupts sleep initiation and maintenance (Özkan & Rathfisch, 2018, Sanlı et al., 2022; Wang et al., 2025; Gueguen et al., 2021; Atis & Rathfisch, 2018). From a biopsychophysiological perspective, these processes may collectively contribute to sleep regulation by reducing both somatic and cognitive contributors to insomnia during late pregnancy. The incorporation of positive affirmations may further support emotional safety, self-efficacy, and adaptive coping processes known to influence sleep-related cognitive patterns (Vázquez-Lara et al., 2025; Siregar & Panggabean, 2024; Islami & Hardjanti, 2022).
In particular, affirmation-based cognitive reframing may help reduce anticipatory anxiety and maladaptive thought patterns that interfere with sleep, thereby complementing physiological relaxation mechanisms. Although physiological mechanisms were not directly assessed in this pilot study, the observed response trends are theoretically aligned with established psychophysiological models linking autonomic regulation, emotional processing, and sleep outcomes. Additional applied and quasi- experimental studies suggest potential roles of hypnotherapy and complementary interventions in improving maternal comfort and sleep-related outcomes (Naz et al., 2024; Panduragan & Pardi, 2026; Siregar & Panggabean, 2024).
Importantly, the digital self-guided delivery model offers practical advantages in terms of accessibility, scalability, and reduced dependence on provider-delivered interventions. Prior research on audio- guided and digital relaxation tools has demonstrated good acceptability within maternal health contexts (Li et al., 2025; Wang et al., 2025; Cheung et al., 2023; Santiváñez-Acosta et al., 2020; Zainiyah et al., 2024). The present findings therefore provide preliminary indications supporting the feasibility of integrating low-resource digital relaxation interventions into routine antenatal care, particularly in community and resource-constrained settings.
Preliminary Patterns in Psychological Readiness for Childbirth
Psychological readiness for childbirth was explored as an additional outcome reflecting maternal emotional preparedness within this pilot framework. Participants engaging with the self-guided digital hypnorelaxation program showed modest short-term shifts toward higher levels of preparedness, whereas changes within the comparison group remained limited. These findings should be interpreted cautiously as early indications of responsiveness rather than definitive improvements in psychological readiness. Existing literature consistently highlights strong interconnections between sleep quality, emotional regulation, and childbirth preparedness. Antenatal sleep disturbances and anxiety are associated with diminished psychological readiness and heightened fear of childbirth (Özkan & Rathfisch, 2018, Nasiri et al., 2018; Chamine et al., 2018; Indahwati et al., 2023). Improvements in sleep are conversely linked to enhanced emotional stability, coping capacity, and self-regulation core components of childbirth preparedness.
The concurrent response patterns observed in both sleep-related well-being and psychological readiness in this study suggest a potentially interconnected relationship, whereby improvements in physiological relaxation and sleep may indirectly support emotional preparedness. However, causal pathways cannot be established within the current pilot design. Relaxation- and hypnosis-based interventions have previously been reported to be associated with reductions in childbirth-related anxiety and improvements in psychological readiness. Systematic reviews indicate that antenatal hypnosis may contribute to emotional preparedness and more positive childbirth experiences (Downe et al., 2015; Catsaros & Wendland, 2020; Gueguen et al., 2021; Atis & Rathfisch, 2018). Affirmation- based strategies further may contribute by supporting self-efficacy and positive cognitive framing related to labor (Vázquez-Lara et al., 2025; Noorlinda & Sartika, 2025; Siregar & Panggabean, 2024; Islami & Hardjanti, 2022).
Compared with previous studies, the present research suggests the potential contribution of integrating multiple regulatory components physiological relaxation, cognitive reframing, and affirmation-based reinforcement within a single, standardized, self-guided digital intervention. This integrated and scalable approach may represent a meaningful extension of existing intervention models, although further investigation is required to confirm its effectiveness. Additional evidence from quasi-experimental and applied clinical studies also suggests potential roles of hypnotherapy and complementary interventions in improving maternal psychological outcomes (Naz et al., 2024; Siregar & Panggabean, 2024). Furthermore, complementary non-pharmacological strategies, including music-based and culturally adapted relaxation interventions, have been reported to support maternal comfort and psychological well-being during pregnancy (Cheung et al., 2023; Santiváñez-Acosta et al., 2020; Zainiyah et al., 2024). Overall, the findings align with existing theoretical and empirical literature while emphasizing feasibility and early responsiveness rather than confirmed intervention effects, consistent with the developmental pilot nature of the study.
Implications for Pilot Development and Future Research
Consistent with its developmental objectives, this pilot study provides preliminary evidence of feasibility, adherence, and early response patterns associated with a self-guided digital hypnorelaxation and affirmation program for women in late pregnancy. The high adherence rates and observed short-term responsiveness across outcomes support the practical feasibility of a digitally delivered, independently usable intervention within routine antenatal care settings. Rather than establishing effectiveness, these findings inform intervention refinement, outcome sensitivity, and study procedures to guide the design of future randomized controlled trials. Importantly, this study contributes to the growing field of digital maternal health by introducing a standardized, self-guided hypnorelaxation model tailored for late pregnancy, addressing a gap in scalable, low-resource interventions. Compared with provider-led or group-based approaches, the present digital format offers enhanced accessibility and potential for wider implementation, particularly in resource-constrained settings.
Limitation
Several limitations should be acknowledged. The non-randomized quasi-experimental design may introduce selection bias, as group allocation was not fully randomized. Although baseline comparability was assessed, residual confounding cannot be ruled out. The sample size was relatively small and consistent with pilot study methodology, which limits statistical power and generalizability. The intervention duration was short (14 days), capturing only immediate response patterns without assessing long-term sustainability. Outcome measures were based on self-reported instruments and may be subject to reporting bias and social desirability effects. In addition, adherence was monitored using self-reported logs, which may introduce potential reporting bias. Despite these limitations, the study provides important preliminary insights into feasibility, adherence, and early responsiveness, supporting the need for larger randomized studies with longer follow-up to establish effectiveness and causal relationships.
Conclusion
This developmental pilot study developed and preliminarily evaluated a self-guided digital hypnorelaxation program integrating guided relaxation and positive affirmations for women in late pregnancy. The findings indicate feasibility, high adherence, and early signals of responsiveness in sleep-related well-being and psychological readiness for childbirth, rather than evidence of clinical effectiveness. These results provide an initial empirical basis to inform intervention refinement, outcome selection, and study procedures for future randomized controlled trials. The scalable and low-resource digital format highlights the potential of this intervention as an accessible supportive component within antenatal care, pending further evaluation in adequately powered studies.
Instruction for AI Assistance Declaration
The author hereby declares that, during the preparation of this manuscript, generative AI tools such as ChatGPT, Microsoft Copilot, and Google Gemini were utilized to assist with language enhancement and grammar correction. Following the use of these tools, the author thoroughly reviewed and revised the content and takes full responsibility for the final version of the manuscript, ensuring its accuracy and adherence to the required academic standards.
Conflict of Interest
The authors declare that there are no conflicts of interest related to this study.
Acknowledgement
The authors would like to thank the participating antenatal care centers and all pregnant women who generously contributed their time to this study. The authors also acknowledge the technical support provided by the digital development team involved in preparing the audio intervention.
References
Abera, M., Hanlon, C., Daniel, B., Tesfaye, M., Workicho, A., Girma, T., Wibaek, R., Andersen, G. S., Fewtrell, M., Filteau, S., & Wells, J. C. K. (2024). Effects of relaxation interventions during pregnancy on maternal mental health, and pregnancy and newborn outcomes: A systematic review and meta- analysis. PloS One, 19(1), e0278432. https://doi.org/10.1371/journal.pone.0278432
Afriyanti, A., Ni'mah, I., Maini, N., Suryani, Y., Irma, Y., & Pradana, A. A. (2021). Efektivitas pemberian hypnosis dalam implementasi keperawatan [The effectiveness of administering hypnosis in nursing implementation]. https://doi.org/10.13140/RG.2.2.12123.44324
Akinwaare, M. O., & Oluwatosin, O. A. (2023). Effect of goal-oriented prenatal education on birth preparedness, complication readiness and institutional delivery among semi-urban pregnant women in Nigeria: A quasi-experimental study. PLoS One, 18(7), e0289414. https://doi.org/10.1371/journal.pone.0289414
Atis, F. Y., & Rathfisch, G. (2018). The effect of hypnobirthing training given in the antenatal period on birth pain and fear. Complementary Therapies in Clinical Practice, 33, 77-84. https://doi.org/10.1016/j.ctcp.2018.08.004
Catsaros, S., & Wendland, J. (2020). Hypnosis-based interventions during pregnancy and childbirth and their impact on women's childbirth experience: A systematic review. Midwifery, 84, 102666. https://doi.org/10.1016/j.midw.2020.102666
Chamine, I., Atchley, R., & Oken, B. S. (2018). Hypnosis intervention effects on sleep outcomes: a systematic review. Journal of Clinical Sleep Medicine, 14(2), 271-283. https://doi.org/10.5664/jcsm.6952
Cheung, P. S., McCaffrey, T., Tighe, S. M., & Mohamad, M. M. (2023). Music as a health resource in pregnancy: A cross-sectional survey study of women and partners in Ireland. Midwifery, 126, 103811. https://doi.org/10.1016/j.midw.2023.103811
Downe, S., Finlayson, K., Melvin, C., Spiby, H., Ali, S., Diggle, P., ... & Williamson, M. (2015). Self‐ hypnosis for intrapartum pain management in pregnant nulliparous women: A randomised controlled trial of clinical effectiveness. BJOG: An International Journal of Obstetrics & Gynaecology, 122(9), 1226- 1234. https://doi.org/10.1111/1471-0528.14403
Eliyawati. (2024). Pengaruh self hypnosis terhadap penurunan kecemasan pada ibu hamil trimester III dalam menghadapi persalinan [The effect of self-hypnosis on reducing anxiety in pregnant women in the third trimester when facing childbirth]. WOMB Midwifery Journal, 3(1), 27–33. https://doi.org/10.54832/wombmidj.v3i1.335
Fernández-Gamero, L., Reinoso-Cobo, A., Ruiz-González, M. D. C., Cortés-Martín, J., Muñóz Sánchez, I., Mellado-García, E., & Piqueras-Sola, B. (2024). Impact of Hypnotherapy on fear, pain, and the birth experience: A Systematic Review. Healthcare (Basel, Switzerland), 12(6), 616. https://doi.org/10.3390/healthcare12060616
Gueguen, J., Huas, C., Orri, M., & Falissard, B. (2021). Hypnosis for labour and childbirth: A meta- integration of qualitative and quantitative studies. Complementary Therapies in Clinical Practice, 43, 101380. https://doi.org/10.1016/j.ctcp.2021.101380
Indahwati, L., Azzahra, S. S., & Indrawan, I. W. A. (2023). Pengaruh self hypnosis terhadap kualitas tidur ibu hamil trimester III [The effect of self-hypnosis on the sleep quality of pregnant women in the third trimester]. Jurnal Ilmiah Kesehatan Media Husada, 12(2), 165-171. https://doi.org/10.33475/jikmh.v12i2.358
Islami, A. I., & Hardjanti, T. S. (2022). Hypnotherapy can reduce anxiety score in high-risk pregnant women. Jurnal Kebidanan dan Kesehatan Tradisional, 11-17. https://doi.org/10.37341/jkkt.v0i0.296
Jannah, N., & Selvarajh, G. (2026a). Development and Pilot Testing of a Childbirth Readiness Questionnaire (CRQ) for Third-Trimester Pregnant Women in Indonesia. International Journal of Public Health Excellence (IJPHE), 5(2), 1–8. https://doi.org/10.55299/ijphe.v5i2.1739
Jannah, N., & Selvarajh, G. (2026b). Multidimensional structure of maternal sleep quality in the third trimester: Psychometric evaluation. International Journal of Public Health Excellence (IJPHE), 5(2), 47– 54. https://doi.org/10.55299/ijphe.v5i2.1798
Li, W., Ren, T., Xu, G., & Wang, Y. (2025). Evaluating the impact of a multimodal perinatal education program on birth preparedness, mental health, and birth outcomes among rural primiparous women: a retrospective cohort study. BMC Pregnancy and Childbirth, 25(1), 56. https://doi.org/10.1186/s12884- 025-07152-8
Manesh, B. K., Tafazoli, M., Fathi, M., Mazloum, S. R., & Moridi, A. (2025). The efficacy of self-hypnosis on sleep quality in the third trimester of pregnancy in primiparous women: A Randomized Clinical Trial. Journal of Midwifery & Reproductive Health, 13(1). https://doi.org/10.22038/jmrh.2023.69364.2040
Montgomery, R. (2025). Sample size justification in feasibility studies: Moving beyond published guidance. Pilot and Feasibility Studies, 11, 88. https://doi.org/10.1186/s40814-025-01675-9
Nasiri, S., Akbari, H., Tagharrobi, L., & Tabatabaee, A. S. (2018). The effect of progressive muscle relaxation and guided imagery on stress, anxiety, and depression of pregnant women referred to health centers. Journal of Education and Health Promotion, 7(1), 41. https://doi.org/10.4103/jehp.jehp_158_16
Naz, S., Khatoon, Z., Karim, S., Atiq, M., & Khattak, I. U. (2024). Effectiveness of hypnobirthing in reducing anxiety level among pregnant women during childbirth: A quasi-experimental study in Tertiary Care Hospital of Islamabad. Journal of Health and Rehabilitation Research, 4(1), 1569-1573. https://doi.org/10.61919/jhrr.v4i1.657
Noorlinda, N., & Sartika, S. (2025). Effectiveness of Hypnobirthing for reducing anxiety before childbirth in third trimester primigravida: A quantitative study in Indonesia. Journal of Current Health Sciences, 5(2), 123–130. https://doi.org/10.47679/jchs.2025124
Özkan, S. A., & Rathfisch, G. (2018). The effect of relaxation exercises on sleep quality in pregnant women in the third trimester: A randomized controlled trial. Complementary Therapies in Clinical Practice, 32, 79–84. https://doi.org/10.1016/j.ctcp.2018.05.008
Panduragan, S. L., & Pardi, K. (2026). Effectiveness of hypnobirthing, music therapy and combined intervention in reducing low back pain among third-trimester pregnant women: A quasi-experimental study. F1000Research, 14, 868. https://doi.org/10.12688/f1000research.168854.2
Paulino, D. S. M., Borrelli, C. B., Faria-Schützer, D. B., Brito, L. G. O., & Surita, F. G. (2022). Non- pharmacological interventions for improving sleep quality during pregnancy: A systematic review and meta-analysis. Revista Brasileira de Ginecologia e Obstetrícia/RBGO Gynecology and Obstetrics, 44(08), 776-784. https://doi.org/10.1055/s-0042-1746200
Sanlı, Y., Goke Arslan, G., Aypar Akbag, N. N., Canbulat Sahiner, N., Yılmaz, D., & Yucel, S. C. (2022). Effects of music on sleep quality and comfort levels of pregnant women. Journal of Perinatal Medicine, 50(4), 467-475. https://doi.org/10.1515/jpm-2021-0551
Santiváñez-Acosta, R., Tapia-López, E. D. L. N., & Santero, M. (2020). Music therapy in pain and anxiety management during labor: A systematic review and meta-analysis. Medicina, 56(10), 526. https://doi.org/10.3390/medicina56100526
Siregar, M., & Panggabean, H. W. (2024). Reducing Effect of Hypnotherapy Anxiety in Pregnant Women. Jurnal Penelitian Pendidikan IPA, 10(SpecialIssue), 482-488. https://doi.org/10.29303/jppipa.v10iSpecialIssue.7828
Teresi, J. A., Yu, X., Stewart, A. L., & Hays, R. D. (2022). Guidelines for designing and evaluating feasibility pilot studies. Medical Care, 60(1), 95–103. https://doi.org/10.1097/MLR.0000000000001664
Totton, N., Lin, J., Julious, S. A., Zhang, J., & Walters, S. J. (2023). A review of sample sizes for UK pilot and feasibility studies on the ISRCTN registry from 2013 to 2020. Pilot and Feasibility Studies, 9, 188. https://doi.org/10.1186/s40814-023-01416-w
Vázquez-Lara, M. D., Ruger-Navarrete, A., Mohamed-Abdel-Lah, S., Gómez-Urquiza, J. L., Fernández- Carrasco, F. J., Rodríguez-Díaz, L., Caparros-Gonzalez, R. A., Palomo-Gómez, R., Riesco-González, F. J., & Vázquez-Lara, J. M. (2025). The Impact of Mindfulness Programmes on Anxiety, Depression and Stress During Pregnancy: A Systematic Review and Meta-Analysis. Healthcare, 13(12), 1378. https://doi.org/10.3390/healthcare13121378
Wang, J., Yang, Q., Cui, N., Wu, L., Zhang, X., Sun, Y., ... & Cao, F. (2025). Effectiveness and mechanisms of a digital Mindfulness–Based intervention for subthreshold to clinical insomnia symptoms in pregnant women: randomized controlled trial. Journal of Medical Internet Research, 27, e68084. https://doi.org/10.2196/68084
Werner, A., Wu, C., Zachariae, R., Nohr, E. A., Uldbjerg, N., & Hansen, Å. M. (2020). Effects of antenatal hypnosis on maternal salivary cortisol during childbirth and six weeks postpartum-A randomized controlled trial. PloS One, 15(5), e0230704. https://doi.org/10.1371/journal.pone.0230704
Zainiyah, Z. Z., Hapsari, V. D., Fitriah, F., & Hasinuddin, M. H. M. (2025). Islamic Sleep Ritual Activity (ISRA) intervention improving sleep quality, physical and psychological comfort for pregnant women in the third trimester. Jurnal Kebidanan, 15(1). https://doi.org/10.33023/jurkeb.v14i1.11921
Phase
Component
Duration
Objective
Example Script
Phase I
Diaphragmatic Breathing
3–5
minutes
Initiate physiological relaxation through controlled breathing
“Now, sit or lie down comfortably… Take a slow breath through your nose… hold briefly… exhale slowly through your mouth… Feel your abdomen rise as you inhale and fall as you exhale… Each breath brings calmness… each exhale releases tension…”
Phase II
Progressive Muscle Relaxation
5–7
minutes
Reduce muscle tension and promote full-body relaxation
“Bring your attention to your body… Start from your feet… release tension… Calves… thighs… abdomen… chest… shoulders… arms… hands… neck… face… Let your entire body feel light, warm, and relaxed…”
Phase III
Guided Hypnotic Relaxation & Imagery
5–7
minutes
Reduce cognitive hyperarousal and enhance mental calmness
“Imagine yourself in a peaceful place… safe and comfortable… Perhaps at the beach or in a quiet garden… Feel a gentle breeze… Your mind becomes calm… All worries drift away… You are safe… You are calm…”
Phase IV
Positive Affirmations
3–5
minutes
Strengthen self- efficacy, emotional calmness, and childbirth readiness
“My body is capable of supporting a healthy pregnancy… I feel calm and relaxed as I prepare for sleep… I trust myself… I am confident and ready for childbirth… I am strong… I am capable… I am ready…”
Closing
Closing Relaxation
±1 menit
Relaxation
“Stay in this calm state… Take a slow breath… When you are ready, gently open your eyes… feeling relaxed, refreshed, and at ease…”
Characteristic
Intervention (n=35)
Control (n=25)
Age (years)
<25
9 (25.7%)
5 (20.0%)
25–35
19 (54.3%)
15 (60.0%)
>35
7 (20.0%)
5 (20.0%)
Gravidity
Primigravida
16 (45.7%)
10 (40.0%)
Multigravida
19 (54.3%)
15 (60.0%)
Occupation
Employed
14 (40.0%)
12 (48.0%)
Homemaker
21 (60.0%)
13 (52.0%)
Education Level
Low
12 (34.3%)
7 (28.0%)
Middle
14 (40.0%)
12 (48.0%)
Higher
9 (25.7%)
6 (24.0%)
Adherence Level
Sessions Completed
n
%
High–Moderate
24–28
30
85.7
Minimum
20–23
5
14.3
Group
Pre-test Mean ± SD
Post-test Mean ± SD
Mean Change
p-value
Intervention
17.3 ± 2.1
8.9 ± 2.0
8.40
<0.001
Control
17.6 ± 2.3
17.3 ± 2.4
0.30
0.326
Category
Intervention
Control
Pre
Post
Pre
Post
Poor
9 (25.7%)
0 (0%)
8 (32.0%)
8 (32.0%)
Fair
26 (74.3%)
0 (0%)
17 (68.0%)
16 (64.0%)
Good
0 (0%)
30 (85.7%)
0 (0%)
1 (4.0%)
Very good
0 (0%)
5 (14.3%)
0 (0%)
0 (0%)
Group
Median (IQR)
p-value
Pre-test
Post-test
Intervention
4 (3–5)
12 (11–14)
<0.001
Control
4 (3–5)
5 (4–7)
0.264
Category
Intervention
Control
Pre
Post
Pre
Post
Low
26 (74.3%)
0 (0%)
18 (72.0%)
17 (68.0%)
Moderate
9 (25.7%)
5 (14.3%)
7 (28.0%)
8 (32.0%)
High
0 (0%)
30 (85.7%)
0 (0%)
0 (0%)